Yogic agnisara increases blood flow in the superior mesenteric artery
Minvaleev RS1, Bogdanov RR2, Bahner D3, Levitov A4, Kuznetsov AA5
1St. Petersburg State University, Saint Petersburg, Russia
2Moscow Regional Research Clinical Institute. MF Vladimirsky , Moscow, Russia
3The Ohio State University Wexner Medical Centre, USA
4Eastern Virginia Medical School, USA
5Pavlov University, Saint Petersburg, Russia
Abstract
Objectives: Medieval yoga texts claim that a special exercise of the muscles of the anterior abdominal wall, called agnisara, improves digestive function. Main objective of the study was to demonstrate change in the blood flow through superior mesenteric artery (if any) after performance of agnisara.
Methods: Ultrasound examination of the linear and volumetric indicators of blood flow in the superior mesenteric artery (SMA) before and after performing the agnisara yoga exercise 100 times was carried out in 12 healthy volunteers of both sexes (8 of them women).
Results: A significant increase in the diameter of the SMA, peak systolic and diastolic velocities, and blood flow in the superior mesenteric artery after performing the agnisara exercise 100 times was found, which contrasts with the established data on a decrease in splanchnic blood flow in humans in response to normal physical activity.
Conclusion: Properly performed agnisara increases blood flow to the splanchnic region, registered by the SMA, which should contribute to adequate blood supply to the gastrointestinal tract for successful performance of digestive function.
Keywords: ultrasound Doppler flowmetry, superior mesenteric artery, exercise, agnisara, uddiyana bandha
Introduction
In the course of our ultrasound studies of yogic postural influences on intracardiac (Minvaleev et al 1996) and intraorganic blood flow (Minvaleev et al 1998, 1999), we decided to evaluate the blood flow to the gastrointestinal tract during the agnisara, or vahnisara, yoga exercise, since in medieval texts on yoga a direct influence on gastrointestinal function is attributed to this exercise (Mallinson 2004). Consequently, modern guidelines for yoga practice repeat the above instruction and many yoga practitioners believe they are increasing their digestive activity, that, however, needs objective verification.
The activation of the digestive tract function must be accompanied and is, indeed, accompanied by a natural increase in its blood supply, which is well established in case of postprandial blood flow to the intestinal region by various independent methods (Norryd et al 1975; Moneta et al 1988), including Doppler flowmetry (Lilly et al 1989). The superior mesenteric artery (SMA), which supplies the whole of small intestine, is often studied, because the anatomy of this vessel lends itself to examination by a noninvasive Doppler ultrasound method (Jäger et al 1986). The adapting of noninvasive Doppler techniques has made it possible to develop reproducible measurements of celiac and superior mesenteric arteries blood flow, which are the main contributors to the gastrointestinal vasculature (Chaudhuri et al 1991).
In a recent study of cerebral blood flow during inverted yoga pose (shirshasana), we found a decrease in the blood flow to the brain through the internal carotid artery, contrary to the prevailing opinion among yoga practitioners (Minvaleev et al 2019), which makes the problem statement relevant for testing other yoga practices. Since it remains unclear how agnisara increases digestive function while physical exercise in general reduces splanchnic and mesenteric blood flow by distributing cardiac output in favor of working skeletal muscles (Perko et al 1998), we decided to evaluate celiac blood flow using ultrasound examination of the SMA before and after doing the agnisara exercise multiple (100) times.
Compliance with Ethical Standards
This study was approved by the Institutional Review Board of Saint Petersburg State University (IRB00003875, irb@spbu.ru). Written informed consent was translated into all relevant languages and cross translated to assure accuracy. Consent was signed by all participants after all questions had been answered by the scientific team.
Subjects and methods
A total of 12 healthy volunteers of both sexes (including 8 women) at the age from 34 to 57 years old were examined (see Table 1 for details).
Table 1. Descriptive characteristics of the test group.
|
No. |
Sex |
Age, yr |
Height, cm |
Weight, kg |
BMI |
|
1 |
m |
45 |
184 |
86 |
25.40 |
|
2 |
m |
48 |
185 |
100 |
29.22 |
|
3 |
m |
41 |
168 |
65 |
23.03 |
|
4 |
m |
53 |
182 |
80 |
24.15 |
|
5 |
f |
44 |
165 |
70 |
25.71 |
|
6 |
f |
57 |
178 |
75 |
23.67 |
|
7 |
f |
38 |
165 |
52 |
19.10 |
|
8 |
f |
34 |
174 |
54 |
17.84 |
|
9 |
f |
49 |
167 |
58 |
20.80 |
|
10 |
f |
51 |
175 |
75 |
24.49 |
|
11 |
f |
47 |
162 |
75 |
28.58 |
|
12 |
f |
47 |
170 |
66 |
22.84 |
|
Mean (SD) |
46.2 (6.4) |
172.9 (7.9) |
71.3 (13.7) |
23.74 (3.4) |
|
All subjects had varying levels of yoga experience and were trained to do the agnisara exercise, each with their own teachers, before starting the study.
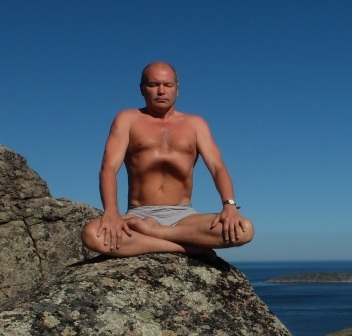
Fig.1 Agnisara
A short description of this exercise is presented, for example, in the medieval instruction on yoga practice called "Gheranda-samhita" (Mallinson 2004, Chapter 1. 18-20): "Move the navel plexus to the spinal column one hundred times. This gets rid of intestinal diseases and increases the digestive fire. This Vahnisara (Agnisara) brings about success in Yoga for yogis…”. Outwardly, it looks like alternate, forceful retractions and protrusions of the abdominal wall, performed along a 20-30 s period of apnea after a full exhalation (Fig. 1). Interestingly, an outwardly similar exercise called "vacuum" has become widespread in Western training systems such as fitness and bodybuilding, with a direct indication that this exercise is adopted from yoga (Rebullido & Chulvi-Medrano 2018) (Fig. 2).
Fig,2 Vacuum exercise.
We performed ultrasound examination of the blood flow of the superior mesenteric artery using an expert class ultrasound machine Fujifilm Sonosite Edge (Bothell, Washington). For sagittal visualization of the abdominal aorta and the superior mesenteric artery extending from it, a C60x convex probe with a scanning frequency of 2-5 MHz was used (Fig. 3).

Fig.3 Ultrasound visualization of SMA.
Protocol
Power and Pulsed Wave Doppler flowmetry of the superior mesenteric artery blood flow was consistently carried out in all subjects in the morning on an empty stomach in the supine position with knees bent to relax the abdominal muscles. All measurements of the diameter of vessels, linear and volumetric indicators of blood flow were carried out during the breath retention of the subjects, which they performed at the request of the researcher in order to avoid the influence of respiratory fluctuations (Seidl H et al. 2010). Power Doppler was used to confirm vascular flow and angle of SMA takeoff. Pulsed Wave Doppler was used to generate a spectral image of flow in SMA at takeoff. Waveform generated and assessed for quality (Quality was determined by lack of spectral broadening in arterial wave form). Scale was adjusted to fit wave form onto image display. Quality image and Doppler wave form with arterial pattern is obtained within 1 cm of SMA takeoff. Calipers are used to measure peak systole and peak diastole. The ultrasound system provides automatic calculation of blood flow by vessel diameter measurement and the velocity time integral. Former is measured by calipers at the target location. Calculation function is used to measure the SMA diameter at the area where Doppler wave form obtained at SMA take off. Volume flow was calculated by measuring peak to peak and converted to ml/min. Further, to assess the resistance in the pulsating vascular system, the resistance index (RI or Pourcelot index) was calculated using the well-known formula:
RI=(PSV-EDV)/PSV,
where PSV - peak systolic velocity and EDV - end-diastolic velocity.
In general, ultrasound examination of baseline blood flow in the SMA in the supine position took no more than 5 minutes. Immediately after this, each subject, in a sitting position with their legs crossed, performed the agnisara exercise, holding their breath after a full exhalation, as many times as possible (Fig. 1). In total, three to four exercise cycles were performed each time after a new exhalation, in order to obtain a total of 100 propulsive movements of the anterior abdominal wall, which took about 2 minutes on average. Immediately after completing the agnisara exercise 100 times, the ultrasound of the SMA blood flow was repeated.
The results of measuring the actual diameter (in cm), peak velocities at the times of systole and diastole (in cm/s), and the total estimate of the volumetric blood flow (in ml/min) in the superior mesenteric artery were read from the obtained sonograms (Fig. 4).
Statistical processing of the numerical results obtained was carried out using the paired samples t test.
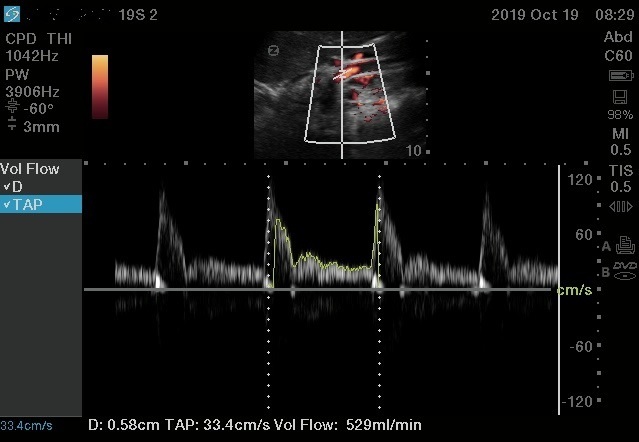
Fig. 4. Typical sonogram of linear and volumetric blood flow in the superior mesenteric artery after performing the agnisara exercise.
Results
At the initial stage of the examination, unidirectional changes in SMA blood flow were found in response to performing the agnisara exercise 100 times in most subjects, which made it possible to draw a preliminary conclusion about an increase in linear and volumetric parameters of SMA blood flow after this exercise. However, in the test subject No.7, in response to performing the agnisara exercise 100 times, a decrease in diameter and an almost twofold decrease in volumetric blood flow in the SMA was discovered. After conversations with her and with other participants, it turned out that their techniques of performing agnisara were different. Namely, subject No.7 performed agnisara in strict accordance with the instructions given in the Gheranda Samhita, pressing the front abdominal wall against the spine, while the rest of the participants, who had received yoga training from another trainer, performed uddiyana bandha (Sanskrit: ’flying up’), in which the front abdominal wall is pulled not to the spine, but up to the diaphragm raised while holding the breath after exhalation (see Fig. 1) before each propulsive movement of the anterior abdominal wall (agnisara proper). On the next day, during the repeated ultrasound examination, subject No.7 performed uddiyana bandha before each abdominal retraction, and the direction of changes in SMA blood flow after performing agnisara 100 times was equal to that of the main group (see Table 2).
Table 2. Indicators of linear and volumetric blood flow before and after the subject No.7 performed agnisara 100 times without uddiyana bandha and with uddiyana bandha.
|
Показатели |
Agnisara |
|||
|
without Uddiana |
with Uddiana |
|||
|
before |
after |
before |
after |
|
|
Diameter, cm |
0.67 |
0.57 |
0,58 |
0,65 |
|
Peak systolic velocity, cm / s |
100.1 |
73.2 |
127.4 |
196 |
|
End-diastolic velocity, cm / s |
16.7 |
24.2 |
24.8 |
36.6 |
|
Volumetric blood flow, ml / min |
634 |
372 |
529 |
864 |
|
Direction of change |
Decrease |
Increase |
||
Since all other subjects (n = 11) performed the agnisara yoga exercise with the preliminary performance of uddiyana bandha, their measurement results, including the results of repeated measurements in subject No.7, were summarized in Table 3 and subjected to statistical processing.
Table 3. Indicators of linear and volumetric blood flow in the superior mesenteric artery before and after the performance by all subjects (n = 12) of the yoga exercise agnisara with the preliminary uddiyana bandha 100 times.
|
Indicator |
Mean (Standard Deviation) |
Probability of the Type I error, α or |
Power for α=0.05 |
Probability of the Type II error, β |
|
|
before |
after |
||||
|
Diameter, cm |
0.605 (0.062) |
0.647 (0.049) |
0.01379 |
0.75928 |
0.24072 |
|
Peak systolic blood flow, cm/s |
144.3 (63.5) |
162.6 (59.4) |
0.3911 |
0.56925 |
0.43075 |
|
End-diastolic blood flow, cm/s |
20.05 (8.64) |
26.88 (9.4) |
0.00336 |
0.92271 |
0.07729 |
|
Blood flow volume, ml/min |
447.75 (323) |
590.42 (351.5) |
0.00228 |
0.94803 |
0.05197 |
|
Resistance index |
0.85016 (0.037) |
0.82834 (0.036) |
0.13638>0.05 |
0.31227 |
0.68773 |
Following the guidelines, we give 95% confidence intervals (CI) for significant changes in the studied indicators:
mean difference in diameter was 0.04 cm (95% CI 0.073 – 0.01 cm) or 6.6% mean increase;
mean difference in systolic blood flow in the SMA was 18.31 cm/s (95% CI 35.5 - 1.1 cm/s) or 12.7% mean increase;
mean difference in diastolic blood flow in the SMA was 6.8 cm/s (95% CI 2.8 - 10.9 cm/s) or 34% mean increase;
mean difference in blood flow volume in the SMA was 142.7 ml/min (95% CI 63.2 – 222.2 ml/min) or 31% mean increase.
Discussion
Table 3 shows a significant (with a probability of type 1 error less than 0.05) increase in all indicators of linear and volumetric blood flow through the SMA after the 100-fold execution of a specific agnisara exercise, despite the statistical invariance of the resistance index (highlighted in gray in Table 3). The revealed absence of a statistically significant change in the resistivity index indicates that the mechanical effect of exercise on the arterial bed is unable to change the tone of the intestinal arterioles, and the recorded increase in blood flow is not associated with this effect. Moreover, the amount of blood flowing through the SMA per minute increased with a probability close to 1.
The latter contrasts with the established data on a decrease in mesenteric blood flow in humans in response to various sympatho-adrenal activations, including physical activity. In other words, a performance of the special physical exercise agnisara 100 times should have reduced the blood flow through the superior mesenteric artery, like any other physical activity, which has been found in many studies (Qamar et al 1987; Peters et al 2001; Moses 2005; van Wijck et al 2011). This is exactly what happened in subject No.7 when performing agnisara without uddiyana bandha. When we added the performance of uddiyana bandha before each propulsive movement of the anterior abdominal wall during agnisara, the volumetric flow of arterial blood along the SMA increased (see Table 2), which allows us to indicate a specific retraction of the anterior abdominal wall towards the diaphragm, called in yoga the uddiyana bandha, as a key element for the correct performance of agnisara.
In 2003, we described a shift in the autonomic tone towards the predominance of parasympathetic influences when performing uddiyana bandha (Minvaleev & Ivanov 2003). The same cholinergic reflex mediates an increase in blood flow to the SMA after a meal (Sieber et al 1991). In our opinion, the increase in the mesenteric duct can be mediated by motor-visceral interaction from the anterior abdominal wall to the central part of the vagus nerve, followed by an increase in parasympathetic influences according to the scheme of the well-known Holtz’ reflex. Thus, the correct agnisara reproduces/imitates the vegetative support of the digestive process before meals, preparing the digestive tract to perform its function.
Interestingly, already at the initial stage of digestion, blood flow in the SMA also increased from as early as the first minute after eating in the mouth, that is, even before the chyme entered the intestine (Someya et al 2008). We observed a similar more than 30% increase in blood flow in the SMA when performing the correct agnisara, of course, outside the meal, which allows us to prove the capacity of a correctly performed agnisara to activate gastrointestinal function through an increase in the SMA. Another insight from our data (see table 3) was that the increase in the mesenteric blood flow after a meal was mainly due to an increase in velocity and volume, the increase in the vessel diameter was less important (Sieber et al 1991, p.364).
Thus, an increase in blood flow to the SMA after repeating this yoga exercise 100 times can be seen as a sign of performing the exercise correctly. Then, our ultrasound experimental data can be seen as a confirmation of the ancient description of agnisara as the practice of "kindling the digestive fire" (Mallinson 2004).
Conclusion
Correctly performed agnisara (with the obligatory performance of uddiyana bandha before each propulsive movement of the anterior abdominal wall) increases blood flow to the splanchnic area, by the SMA, which should contribute to an increased blood supply to the gastrointestinal tract accompanying adequate improvement of the digestive function.
Clinical Relevance
Properly performed agnisara increases blood flow to the splanchnic region for successful performance of digestive function. Our results allow us to hope for the use of the agnisara for the prevention of ischemic causes of gastrointestinal problems in athletes.
Acknowledgements
The authors express their heartfelt gratitude to Irina Arkhipova, general director of the film studio of the historical film "Pharaoh", the inspirer and organizer of international scientific expeditions within the framework of her author’s project "In Search of Lost Knowledge" (c), aimed at supporting national science, as well as to all participants of the expeditions "Pyrenees-2018" and "Pyrenees-2019".
References
Chaudhuri KR, Thomaides T, Hernandez P, Alam M, Mathias CJ 1991 Noninvasive quantification of superior mesenteric artery blood flow during sympathoneutral activation in normal subjects. Clinical Autonomic Research 1: 37-42. https://doi.org/10.1007/BF01826056
Jäger K, Bollinger A, Valli C, Ammann R 1986 Measurement of mesenteric blood flow by duplex scanning. Journal of Vascular Surgery 3: 462-469. https://doi.org/10.1067/mva.1986.avs0030462
Lilly MP, Harward TR, Flinn WR, Blackburn DR, Astleford PM, Yao JS 1989 Duplex ultrasound measurement of changes in mesenteric flow velocity with pharmacologic and physiologic alteration of intestinal blood flow in man. Journal of Vascular Surgery 1: 18-25. https://doi.org/10.1067/mva.1989.vs0090018
Mallinson J. 2004 The Gheranda Samhita: the original Sanskrit and an English translation. YogaVidya.com
Minvaleev RS, Kuznetsov AA, Nozdrachev AD, Lavinskiĭ, IuKh 1996 Left Ventricle Filling in Sirshasana and Sarvangasana Yogic Postures. Human Physiology 6: 665-671. Translated from Fiziologiya Cheloveka 6: 27-34
Minvaleev RS, Kuznetsov AA, Nozdrachev AD 1998 The Influence of Body Position on the Blood Flow of Parenchymatous Organs: 1. Liver. Human Physiology 4: 475-480. Translated from Fiziologiya Cheloveka 4: 101-107
Minvaleev RS, Kuznetsov AA, Nozdrachev AD 1999 The Influence of Body Position on the Blood Flow of Parenchymatous Organs: II. Kidneys. Human Physiology 2: 203-209. Translated from Fiziologiya Cheloveka 2: 92-98
Minvaleev RS, Ivanov AI 2003 Uddiyana-bandha. Adaptivnaya fizicheskaya kul’tura. 1: 10-11. (Article in Russian)
Minvaleev RS, Bogdanov RR, Bahner DP, Levitov AB 2019 Headstand (sirshasana) does not increase the blood flow to the brain. Journal of Alternative and Complementary Medicine 8: 827-832. https://doi.org/10.1089/acm.2019.0060
Moneta GL, Taylor DC, Helton WS, Mulholland MW, Strandness DEJr 1988 Duplex ultrasound measurement of postprandial intestinal blood flow: effect of meal composition. Gastroenterology 5: 1294-1301. https://doi.org/10.1016/0016-5085(88)90364-2
Moses FM 2005 Exercise-associated intestinal ischemia. Current Sports Medicine Reports. 4: 91-95. https://doi.org/10.1097/01.csmr.0000306079.74945.ea
Norryd C, Denker H, Superior mesenteric blood flow during digestion in man. Lunderquist A, Olin T, Tylén U 1975 Acta chirurgica Scandinavica 3: 197-202.
Perko MJ, Nielsen HB, Skak C, Clemmesen JO, Schroeder TV, Secher NH 1998 Mesenteric. coeliac and splanchnic blood flow in humans during exercise. The Journal of Physiology 513: 907-913. https://doi.org/10.1111/j.1469-7793.1998.907ba.x
Peters HP, de Leeuw D, Lapham RC, Bol E, Mosterd WL, de Vries WR 2001 Reproducibility of ultrasound blood flow measurement of the superior mesenteric artery before and after exercise. International Journal of Sports Medicine 22: 245–249. https://doi.org/10.1055/s-2001-13811
Qamar MI, Read AE 1987 Effects of exercise on mesenteric blood flow in man. Gut 5: 583-587. https://doi.org/10.1136/gut.28.5.583
Rebullido TR, Chulvi-Medrano I 2018 The abdominal Vacuum technique for bodybuilding. Strength and Conditioning Journal 5: 116-120. https://doi.org/10.1519/ssc.0000000000000434
Seidl H, Tuerck J, Schepp W, Schneider AR 2010 Splanchnic arterial blood flow is significantly influenced by breathing-assessment by duplex-Doppler ultrasound. Ultrasound Med Biol. 10:1677-81. https:// doi.org/10.1016/j.ultrasmedbio.2010.07.017
Sieber C, Beglinger C, Jaeger K, Hildebrand P, Stalder GA 1991 Regulation of postprandial mesenteric blood flow in humans: evidence for a cholinergic nervous reflex. Gut 4: 361-366. https://doi.org/10.1136/gut.32.4.361
Someya N, Endo MY, Fukuba Y, Hayashi N 2008 Blood flow responses in celiac and superior mesenteric arteries in the initial phase of digestion. American journal of physiology. Regulatory, integrative and comparative physiology 6: R1790-6. van Wijck K, Lenaerts K, van Loon LJ, Peters WH, Buurman WA, Dejong CH 2011 Exercise-induced splanchnic hypoperfusion results in gut dysfunction in healthy men. PLoS ONE 7: 22366. https://doi.org/10.1371/journal.pone.0022366
Файлы для скачивания: